Ephesians 4:22-24 says, “…in reference to your former manner of life, you lay aside the old self, which is being corrupted in accordance with the lusts of deceit, and that you be renewed in the spirit of your mind, and put on the new self, which in the likeness of God has been created in righteousness and holiness of the truth.”
I’m curious about that. Can this really happen? Do you become a committed Christian and thennnn, POOF! you’re suddenly a nice guy, ‘filled with righteousness and holiness?’ I think what I’m really asking here is, do people change? It’s a time-honored question, typically followed by the time-honored answer: No.
There’s research on the malleability of personality, or the lack of it. Certainly during a person’s early years there are changes in personality as they move through childhood and adolescence into adulthood. But most parents will tell you that the kid they saw on Day 1 seems a WHOLE LOT like the kid they have on day 10,000. There’s lots of data supporting that the rudiments of personality are “knit together our mother’s womb.” (yep, the Bible makes that case too.)
But we’re not talking about personality change here. In fact, one Biblical scholar I read described this passage as in fact not a command at all. The Apostle Paul (the writer of Ephesians) is using a verb structure here to describe a change, not command a change. He is in effect describing the transformative power of salvation in Jesus Christ.
This guy’s having a GREAT day. Thanks, transformed, holy Christians!
Well, that’s a weird thing to say, isn’t it? Christians are remarkably BAD humans in many contexts especially when viewed across the whole spectrum of history. The inquisition comes to mind. This was an office of The Church (meaning the Roman Catholic version of it) set up in the 12th century meant to root out and punish heresy throughout Europe and the Americas. Nice set of folks, them. Were especially, um, helpful, toward Muslims and Jews. This went on for hundreds of years, too. It wasn’t just the bad idea of one overly powerful guy who eventually got wiped out and then Christians came back around to being kind and holy again.
So, historically, Christians didn’t get it right, much of the time. Here in modern times, it stands to reason we’re still not getting it right. So, are we really transformed when we invite Jesus into our lives?
I think medically, the answer is a qualified yes. Qualified in numerous ways, but let’s discuss one:
How “full” or “true” your initial conversion to Christianity plays a central role in whether or not you actually change when you take on the Love of Jesus in your life. By this, I mean that if you came to Christ because you sat through endless sermons as a kid, forced there by your parents and eventually just figured you were also a Christian, there’s a chance your connection to God is tenuous at best. Hence, the change in your life and heart is likely to be nominal.
By contrast, if you experience a sweeping moment of divine rapture, which happens to a great many people in a great many contexts virtually every day, your life is likely to change dramatically. There’s a standardized test that bears this conclusion out, actually. It’s called the IRES scale (the Intensity of Religious Experience Scale). When a person takes this test and scores high on the Experience of God component, there is evidence to show that person will have a high level of confidence in God, and seek to have a deeper relationship with Him. That person is open to the needs of others and sees their life as meaningful and valuable, accompanied by joy and peace.
I’m gonna go out on a limb here and suggest that those august and sage “Christian” torturers of the Inquisiton, or the myriad weirdo Christians peppered through American culture today who do all kinds of things not found in scripture, would have scored reeeel low on the IRES scale, if at all. In other words, there are genuine encounters with God, and inauthentic ones. Only the former leads to the outcomes described by Paul in Ephesians (and Romans 6:2-10, 2 Corinthians 5:17, among others).
When a child shrieks out in searing pain, you never forget the sound.
“What does he have?” asked my steadfast Haitian translator. I barely paused, though I’d only ever read about the disease in my medical school text books. “Polio,” I said, fighting back a new conglomerate sensation best described as a combination of anxiety, shortness of breath and vertigo.
The boy was 9-years old. He lived with his destitute family in the Haitian village of Noyo, an hour’s hike from the nearest road. His cries were in response to his heroic efforts to stand, as his soiled diaper slid down his cable-stiff legs. He inched forward on his toes, unable to relax his calf or quad muscles, unable to remain continent. His wail turned into a barking gurgle as he inched his way forward.
There are certain smells, sights, sounds that stay with survivors and observers of tragedy. The smell of burning flesh, for example, never leaves you. I learned this from my patients when I worked in the wounded warrior unit in Landstuhl, Germany. But for me, it will always be the awful, persistent sound of a child crying out in abject pain and misery.
“How, in the name of God, do we stop this?” My translator asked.
“Vaccines.” I said. “And, funny you should ask in the name of God. I can’t think of anyone else who gave us the intellectual capacity to invent something, anything, that could stop such horror.”
Here in Washington State just last week, the boy’s pain came to mind as I sat with a patient in my clinic, talking about the flu shot. “I never get the flu shot, doc. Never have,” he said.
“Oh? Why’s that?” I asked.
“I don’t need it,” he said. “In 65 years, I’ve never gotten the flu.”
“I certainly understand your reasoning,” I replied. “You’re effectively choosing empirical data to drive your choice, right?”
“Like, there’s no evidence that I’ve ever gotten the flu?”
“Exactly. Totally reasonable, except that the problem lies in what you can’t sense. There is every possibility you’ve had the flu in your life. Maybe many times. It just didn’t make you very sick.”
“So, same thing: I don’t need a flu shot for something that doesn’t make me sick.”
“Respectfully,” I replied, “It’s not about you.” He looked quizzical. We’ll call him James. He’s a highly intelligent man from what I gather, not accustomed to new data further informing an already-considered opinion.
“It’s not uncommon for viral illnesses to spread before you have symptoms, or to spread when you are infected but never have symptoms at all. This puts the young, the weak, the old, the immunosuppressed at great risk. We don’t want you to get immunized for you. We’re worried about them.”
He gave me a flat stare, “That angle of the vaccine debate is under-emphasized,” he said. “You really should focus on that part of the issue. It was never really clear to me before now.”
If I were to design a pro-vaccine campaign, I’d make simple Signs and T-shirts and stickers. All black, with white letters that say:
It’s Not About You
(Get Vaccinated)
I’m continually surprised to see how many people don’t quite understand the effects of their reasoning regarding vaccines. The idea is to halt disease in the one person you can control – YOU – so that it doesn’t create unmitigated misery in those you can’t control (others). Somehow, this message just isn’t making the rounds.
One theory about why: Maybe Americans don’t really see awful suffering all that much. We think we have a grasp of it but we really don’t. We talk about some in this country being vastly more privileged than others, and to a degree this is true. But it’s worth remembering that all except the very tiny minority of the poorest Americans are vastly more wealthy, protected and privileged than much of the rest of the world. It’s been said that if you have a fridge and a cell phone, you’re rich by definition. And trust me, all but the worst in America is a Country Club compared to Port Au Prince.
I recognize, it IS hard to act on things you can’t see or perceive. And so in this case, despite whatever risks of masks or vaccines, I wish I could bring all my countrymen back to that moment in the crumbling concrete church in the rocky hills of Noyo where we ran our little aid clinic. And while I wouldn’t wish the lingering sounds of those tortured screams on anyone, I do wish I could convey their effect. When you see it, when you hear it, you can’t forget. Within the helpless sorrow of that misery, vaccines are an easy choice.
**Images not used with permission. I hope I don’t get busted here. They DO link to the sites from which I “borrowed” them. I’m trying to do a good thing here; there’s no money headed my way from their use.
Today marks a week since the passing of The Writer’s Almanac, one of the few modern examples of true literary culture edging – just slightly – into the American mainstream.
The Almanac has been around for 24 years. Hosted by its creator, Garrison Keillor, each daily program included vignettes about authors and other noteworthy people whose birthdays or significant events coincided with the date of the particular program. There were also interesting excerpts of important events in history.
The program continued with one or more poems usually chosen and read by Keillor. The show ended with his traditional sign-off, “Be well, do good work, and keep in touch.” The theme music was a version of the Swedish song “Ge mig en dag”, performed by Richard Dworsky on piano.
Keillor has recently been accused of ‘inappropriate conduct’ by a co-worker at Minnesota Public Radio, which has the distribution rights to the show. He has been summarily removed from all his connections to the station, and, among other actions, the Almanac is no more. The details are murky. It isn’t clear what was committed; from crimes against humanity to repugnant boorishness to internecine office politics. But the Almanac is gone. That we know.
This loss is a terrible thing. The Almanac goes quietly, ‘with a whimper,’ but the magnitude of the demise cannot be understated. Thousands of writers, poets especially, saw a small sliver of light fall across their obscure desks because of the Almanac.
Ever heard of Athena Kildegaard? I hadn’t. ‘Till A Mother’s Poem showed up in my email the other day. Same for the poetry of Anne Sexton, Paul Hostovsky, David Romtvedt, Ogden Nash, Janice Moore Fuller, Dorianne Laux and hundreds of others. Each post in the Almanac included links to buy the works of these poets, which I’m sure was a huge benefit to them. Ever tried to sell a poem? Ever tried to keep the heat on in winter with income from your wordcraft? Give it a shot. Have fun.
Another casualty: The Poetry Foundation. Long fighting a valiant Thermopylae-esque battle for the attention of the American public, this beleaguered institution will crumble further into obscurity. Many of those who attempt to live by the spoken or written word will feel the effects of this ignominious end.
I think of all the people who made their living from the show too: The Almanac was written by Betsy Allister, Joy Biles, Priscilla Kinter, Heather McPherson, and Holly Vanderhaar, the program was engineered and edited by Thomas Scheuzger, Noah Smith, and Sam Hudson. Production assistance was by Kathy Roach and Katrina Cicala. I don’t know any of these people, but I presume they’re now using those fabulous writing skills on their resumes.
This is a blow to the English language itself. The Writer’s Almanac invited Americans to spend time with those who are excellent and exacting in their use of English. This, in turn, pushed those of us with lesser skills to be better with the craft. To avoid sentence fragments, for example. And fight the urge to grow wary when in fact we were weary. Great English avoids misconfusing conjunctions. And doesn’t use nouns to modify verbs (e.g. ‘travel safe’ is, ostensibly, a thing, ‘travel safely’ is a well wish). Great English makes whimsical and witty use of alliterations (you be the judge with that one).
But to my way of thinking, the greatest effect of the loss of the Almanac is to the American mind. I’ve long been suspicious of just how well the average American thinks, myself included. I’m dubious that we as a people place a high enough standard how and at what point we decide something is True. America today seems to be a land of sports spectacle and activism, neither of which lend themselves to nuanced and charitable thinking. Intellectual certainty abounds. Justice may rarely roll down like water these days, but arrogance about one’s opinions certainly does.
Poetry tends to avoid absolutes. It remains one of the few places where the dress could be blue, or gold, or both…and still be considered valid. And valuable. A poet once told me that a good poem has two completely different meanings, depending on how it is read – a great poem has three. Poetry demands of us the ability to find both satisfaction and fascination in such unkempt intellectual complexity.
I met my future wife over Faulkner, but things really heated up when Cummings and Frost got involved. To say I owe my marriage, and all the glories that have resulted thereafter, to poetry is both overstatement and understatement. I mean, words…what can they really do for us? No doubt it was actually those relentless brown eyes. Then again, perhaps it was the waves, which did something to the shore that water never did to land before.
It may be that shutting down the Almanac was necessary; the justice of sins come home. Perhaps it is the victim of McCarthyist purges. Either way, the loss is incalculable. The exit of a Today Show anchor or a Hollywood movie producer barely rends the cultural fabric of America. But the loss of The Writer’s Almanac shreds it. All are bereft of so much more than can ever be said. Except, perhaps, by the poets, who are now even more quiet than they were before.
Being a Christian refugee in this part of the world is a dangerous affair.
Unlike in America, where counting oneself a Christian is increasingly perceived as a designation that affords privilege, sometimes to an unfair degree (I have my doubts on that one), there is no question that the opposite is true in much of the Middle East.
It is easy to see that militant Islamists are actively focused on the eradication of Christianity in at least “Muslim” lands, if not the whole world. This is true to some degree in the refugee camps as well.
Even still, many of the refugees we worked with this week are either committed Christians, or are actively exploring the faith.
The stories of how these people came to their decisions for Christianity vary widely, but most are eye-opening. Few in the Middle East can come to Christ as easily and risk-free as nearly every American can if they wish. Apostasy from Islam is often regarded as an offense punishable by death.
One man I saw this week was openly wearing a prominent silver and gold cross around his neck. I didn’t notice it at first, but as I was listening to his heart with my stethoscope the bright golden object swinging in front of me was suddenly hard to miss.
Realizing I wasn’t in America, where crosses are so ubiquitous they’ve become a little trite to me, I exclaimed, “You’re wearing a cross!”
“Yes,” he nodded.
I pondered the implications of wearing that specific symbol in the Islamic world. A cross is better described as cross-hairs for a man like him. Yet he wore the symbol proudly, unapologetically. Should our roles be reversed, would I have the same courage?
“You are a Christian then.” I said, continuing in my new role of Dr. Redundant.
“Yes.” He nodded again, smiling.
Through my translator, I learned that a few months ago in Iran he was awoken in the night by the figure of a man calling him to follow Christ. He said he was convinced that the man speaking to him was Jesus, the Son of God. He knew almost nothing of the Christian faith, as he was raised a Muslim.
Still, upon waking the next day, my patient committed himself for following Christ. He felt he had to do this. It was an inner compulsion; he had been called to a new faith, a new life, no matter the cost to him.
But it was indeed a ‘costly’ decision. Read anything about the Islamic regime of Iran (I recommend the the wonderful autobiography Persepolisas a cursory intro if interested), and you will know that the government of Iran is itself a religious organization. Along with typical functions of any secular government, like providing running water, working roads, electricity and health care (which in many instances, the Iranian government does quite well), it also enforces a highly conservative interpretation of Shia Islam.
How do they enforce such a thing, you ask? How do you get a nation of 77.5 million people to follow extremely strict religious rules? How can you enforce an entire nation to put every woman in robes and headcoverings, to allow no music, no dancing and to enforce frequent observance of Islamic practices like 5x daily prayer?
With “religious police” of course!
As a kid from the suburbs of America, following a Christian faith I was always free to reject, it took some reading and imagination for me to even comprehend such a notion.
It was only in 1979 that the Iranian Revolution took place. Prior to that, Iran probably looked much more like America than it does today. But in ’78-’79, things changed dramatically, as that was the year of the Iranian Revolution. It was then that the Pahlavi dynasty, led by Mohammed Reza Shah Pahlavi was overthrown by the Islamic Republic.
Supporters of the Revolution. Didn’t Turn Out Like Many Expected.
The Republic was initially a political movement, comprised of a collection of leftist thinkers, activist students and numerous Islamic movements. It was led by a powerful Islamic leader named Ruhollah Khomeini, a scholar, author, politician and political revolutionary.
After the Shah was forced from power, to the surprise of nobody, Khomeini was designated as the Supreme Leader of Iran. However, TO the surprise of many, Khomeini was given final authority on both political and religious matters.
The irony of this transformation is hard to miss. Criticism of the Shah centered around how difficult it was for the commoner to be heard. The Shah’s rulership was a dynastic monarchy, with power passing from father to child generation after generation. This meant that nobody could rise from, say, a community organizer and member of a minority comprising 13% of a nation’s population, like Barack Obama, to the highest position of power in the land (Huzzah! Huzzah! Democracy!).
Yet the solution to this problem that emerged in Iran was the Islamic Republic, which consolidated both political and religious power in one man. The power of the rulers of Iran was, effectively, broadened as a result of the revolution. The “little people” never got their say. And, I suspect, many of those who supported the Revolution experienced colossal disappointment. Power just went from one ruling class to another. To this day, a Khomeini rules Iran.
Some version of the above rushed through my mind as I stared at the cross hanging from my patient’s neck. An Iranian, 4 months in Greece, wearing a bright silver and gold cross. Wow.
As it turns out, the father of this man was a member of this religious police force. This patient had chosen to convert from Islam to Christianity as the son of a man who is tasked with enforcing and promulgating Islam in the country. More irony.
Imagine the shame on their family for such an act! Aside from endangering himself, my patient was possibly even endangering his own father (and mother).
Many immigrants come to Europe because they think it is rich, with jobs and money flowing like wine at a wedding party. Increasingly, they are finding that Europe is no utopia. Millions are unemployed. Millions are poor. Upward mobility is rare.
But one reality of Europe is that it does remain a place where you can follow a religion in nearly any any way you choose, to include no religion at all. Say what you will about the EU, but it remains a place of tremendous religious freedom, rivaled perhaps by only the U.S.
So it is understandable that this man left Iran. But it is still amazing that he was willing to do it. He left with nothing. No family, no friends. He slunk away in the night, alone. As the son of an important man, his life had no doubt been comfortable and safe. He upended all of that.
Pireaus Port. Lucky you if you have a tent.
My patient arrived at the Pireaus Port of Athens after crossing the Agean Sea from Turkey. He arrived nearly destitute, having given most of his money to a trafficker to get him to Greece. I think he slept on the concrete sidewalk the first night.
The next morning, he says he prayed that the God of his new faith would spare him, and shortly thereafter was approached by members of a Christian church in Athens who offered him a bottle of water. It was through this church that I met him.
Greek authorities soon placed this man in the Elliniko refugee camp, where he made no secret of his faith, sharing it with any around him who would listen. Not long after his arrival, a riot broke out in the camp with Muslims targeting Christians.
The violence carried on for quite some time, as Greek police made no move to stop it, one even pointing out that if some of the refugees died, “there will be fewer of them for us to deal with.” My patient was beaten severely in the melee.
It is inhumane, of course, for anyone to think as these police did. But their attitude is understandable nonetheless. Would you wade into the middle of that mess?
Somewhere in this story, my patient picked up his cross. I don’t know if it was in Iran or somewhere in Athens. But he wears it daily. It is not merely jewelry to him, given at some Christmas party. It wasn’t bought from one of the ubiquitous Christian Book Stores in America, with every possible permutation of “cross trinkets” available for sale. It was bought for a price; worn for a higher one.
This isn’t necessarily a Christian story, although as a Christian I find it inspiring. But from this anyone can recognize the deep human desire to worship in freedom. This man’s life story is a reminder that people are willing to die for the right to think and act honestly in relation to their understanding of the divine.
The cross symbolizes the reality of this man’s beliefs, even if that symbol marks him for suffering or even death. Would that all Christendom be so committed. Would that all who cherish freedom be so as well.
For the second time in less than a year, I’m on my way back to Athens. This will be a short trip with virtually no team. My colleague organizing things in Athens has stated that she “feels sorry” for me, as the number of people signed up for the clinic appears to be quite large.
From what I can tell, the situation in Greece has only gotten worse since I was last there. Many borders and routes into Europe have closed, and migrants are being turned away at far greater numbers than they were last year. But by “turned away,” I’m not describing from Greece itself. Nope. Thousands continue to arrive on the shores of Greece every day. I’m talking about further into Europe. So, the migrant population continues to swell in Greece, especially Athens. Although authorities have begun shipping back some migrants (numbering in the hundreds) in the past few days, this is a small small number.
I say I’m bringing ‘no team’ this time, but in reality this isn’t accurate. Aside from what sounds like a great number of willing helpers in Athens, I also will bring my 14 and 16 year old daughters with me this time. I don’t know what sort of role they will be able to play in the work we do this time. It could be simply watching the children of the patients while they’re waiting the doc.
Hopefully, they can learn a bit about medical care in a refugee and/or underserved situation. As their lives are largely consumed with cheerleading, skinny jeans, teen-lit, French horn, Cello, soccer and boyfriends (ex…EX boyfriends), this might be quite an eye-opening experience for them. I hope so.
My biggest concern is that we will successfully collect accurate data on the patients we see. Last time we did a fair job, under the circumstances, but in my spare time I’m STILL working through the XL spreadsheet and trying to come up with data summaries that will be of some use to the wider medical world.
This time, I hope to have time to ask better questions, and to formalize how we input the data. It is well known among those who do medical research that 80% of the study is done before the study begins. Developing a means to collect data, to college USEFUL data, and to do it in a way that is searchable and accessible at a later date is difficult. It is especially difficult when at that later date, you are dealing with hundreds, maybe thousands of data points.
I’ve had enough training in this element of the medical world to feel a gnawing sense of anxiety as I approach the issue. My medical school heavily emphasizes epidemiology and biostatistics, and I was part-way through an Master’s in Public Health degree until I ran out of money. So I have a sense for how easy it is to do this stuff badly. But I wish I had a collaborator or better skills to know I could do it well.
Still, I’ve had some help from a colleague at work who maintains a quizzical affection for XL (I can’t judge, I was once in a steady relationship with Photoshop), and he has helped me clean up our data from October. And I have a much better sense for what I need to do this time around.
It should be mentioned that most relief agencies don’t actually do any of this, even the good agencies who actually help people (lots of them are there for the photo-op and little else, it seems). I received some generous help from a professor at the London School for Hygiene and Tropical Medicine prior to my last trip, and he noted only a small number of agencies who provide care AND do good, statistical research on the populations they serve.
So, it makes sense that I’m somewhat on my own here. It’s not easy to focus on research and practical care at the same time, as one is more empathy-driven, the other much more analytical and “cold.”
Example: if someone comes in coughing up blood, you can either turn and enter “hemoptysis” into your spreadsheet (and then get the heck out of there because…ew), or you can throw on some gloves, hopefully a mask, get them on a bed and start working them up for any of the many many possible reasons for that symptom (most of those reasons being prit-TEE bad).
So, we will see how this goes. We leave tomorrow (Sunday) afternoon.
I myself have done relief work in Haiti. One of the places I worked is located in the hills of a village-esque area called Noyau. This place is about as remote from civilized life as I can recall being in my life.
After an hour of 4WD driving on extremely-rough dirt switchbacks up a mountainside, we pulled on packs and hiked for another hour+ to reach the area of our clinic. If something went wrong out there, the time required to receive aid would exceed 4 hours easily. Assuming emergency crews had access to a 4WD vehicle, which is doubtful.
I recall thinking, as well over 100 Hatians stared at us zipping ourselves into our expensive tents and sleeping bags at the end of a clinic day, how honorable they were as a people. They had hiked for many hours to find our clinic, and often the only thing we had to offer them upon their arrival was a few TUMS tablets. Frequently their medical problems were either too complex for us to help with, or, more commonly, we simply didn’t have the medicine or procedural ability they needed.
But they could have robbed us. Selling our nice North Face and Sierra Designs gear would have fetched an impressive price in Port au Prince. Furthermore, they could have kidnapped us and held us for ransom. Now we’re talking real money. Until they talked to my wife, who would probably say something like, “Take ‘im. Never does the dishes anyway.”
We were totally vulnerable in that village. But the reason, I believe, nothing bad happened was simply because most Hatians are good people. Honorable people. Honorable, even, by my wealthy American standards, where respect for property and life is alive and well. They let me keep my nice tent, even though they couldn’t be sure of their next meal.
Similarly, while working in the Galatsia camp on our 3rd day in Athens, I ended up in an extremely vulnerable position. Again, we came out unscathed largely because most people are, quite simply, good.
Prior to entering the camp, I asked one of my team members with military training to effectively serve as our “security.” He took his role seriously: identifying sight-lines, exits, areas of risk, areas of relative safety. He developed rudimentary emergency plans, identified key leaders in the facility and communicated escape plans to our team.
But for some reason, when I was asked to leave our clinic to go see a patient reportedly too sick to walk to us, I didn’t think to ask our security guy to come with us. In “medical mode,” it’s difficult to think in “safety mode” too. Our task is to meet needs, not protect ourselves, and the thinking between the two is often very different.
See all the people? That lady in blue is an aide worker. Behind me was a large room, a courtyard, and a line of police. I thought we were going here.
I also believed we would be going to one of the large rooms with lots of people, located near the entrances, near the police, organizers, aides and managers.
That’s not where we went.
Led by the sick woman’s husband, we walked down corridor after corridor. Branching off from each of the primary hallways were other halls, down which I saw a half-dozen young Middle Eastern men, crouched against the wall, all looking at me. The halls were strewn with trash, cell phones hanging by cords from every available outlet. I heard yelling, some laughing, but mostly saw numerous drawn, emotionless, bored faces. There was no joy.
I went with our clinic organizer (a Persian woman who organized the whole medical clinic, speaks numerous languages, and knows what she’s doing) and, as luck would have it, the pastor of the local Calvary Chapel we’re working with who saw us wandering away and followed. So at least I wasn’t alone.
This happened in the Philippines just last month. However improbable, we could have rounded the corner and found guns and flags, not a patient.
But after the 3rd corridor, and up a large flight of stairs, then outside the building and then back into it and around a corner, I knew that if someone wanted to do us harm, they would have succeeded. We’d followed this guy like ducklings.
But he didn’t harm us. All the man wanted was to know if his wife would be OK, and if it might be possible to get her on her feet by that evening, in hiking condition. He intended to continue his journey into Europe as soon as he could.
I diagnosed viral gastroenteritis and told him she may be ready to roll by that evening, but giving it another day or two would be better. He clearly intended to leave that night, despite what I’d said.
Later, of course, we laughed about this. Our team leader, Sahar, laughed at me for being so worried.
But the truth is that there is no way to do this work without incurring some amount of risk. Usually the risk is small, thanks largely to the fact that although there is terror and violence in the world, most humans on this planet are good, fairly honest people. Most are just trying to make a better life for themselves and their children.
On day 3 we left our makeshift clinic in the 2nd Evangelical Church of Athens to work in one of the main refugee “camps” in town. But it isn’t a campground. It’s one of the main stadia used in the 2004 Olympics, located in the Galatsi suburb of Athens.
The story of how this stadium came to be used for refugees is emblematic of the refugee crisis in generally. The stadium has been shuttered for years, no lights, no electricity. But with thousands of people suddenly camping in parks all over Athens, the people of the city were understandably upset. Furthermore, anti-immigration groups were organizing and preparing potentially-violent opposition to the influx.
So the Minister of Immigration apparently decreed that refugees would be moved to the Olympic Stadium. Only then was the mayor of Galatsi notified of the dictate, while also being told that he was, in fact, in charge of the stadium.
Queuing up for lunch. The food I saw was a step up from David Copperfield-esque porrige, but not by much.
On balance, it’s a good plan. There is lots of room there, the people and tents are out of the parks and off the sidewalks. The Greek Army (I think) has been tasked with feeding the refugees 3x per day, an endeavor equal to any reasonably-trained Army. It also protects Greek political leaders from human rights criticisms, since the people are being cared for while not upending entire neighborhoods.
There is both massive influx and efflux of people from the stadium every day. Nobody intends to stay for long; the Greek government does not plan on operating the facility indefinitely either.
We were given an emergency medical license under which I could function as a de facto Greek doctor on days when I worked at any of the camps. We were asked, really more like begged, to work at the Galatsi camp because over 1000 people were there, with hundreds requesting a doctor.
Here are some observations from that day:
Lots of people, all trying to help. Not a lot of organization.
We worked out of a small room, filled with donated medicines, even some supplies. It was better-appointed than I expected. It was cramped, sweaty and regularly filled with people for myriad reasons. A hazy notion of ‘organization’ came and went throughout the day.
We infuriated the Greek doctor, a pulmonologist, who is overseeing the medical room in the camp. We had been “begged” by the ministry of immigration to come work that day. She was never notified. So our presence was a surprise to her. She wasn’t, however, working. Nobody was. She showed up, yelled at us about attending a strategy meeting in a few days, hung around for a bit, then left.
The Greek Government is doing better with this crisis than reported. There
Areas around Greece where people are helping with the refugee crisis either directly or by collecting donations, etc. Click this pic for an interactive map.
were police on the campus (until later in the afternoon, when they apparently lost interest and wandered away). There were GIANT piles of clothes in the “clothes section,” and everyone had food at mealtimes. The camping areas were dry and were clean if the refugees cleaned up after themselves (some did, some didn’t). But the same Greek Government has relied heavily on individual donors, NGO’s and privately-funded clinics like ours’ to make this some sort of controlled chaos.
Before we started, I watched a T.V. reporter van pull up next to a nice black car, out of which stepped some guy in a suit. The camera started rolling as the guy stood next to a reporter-looking person. There was a quick interview, then some panning shots of the facility. Then the guy got back in his car and drove away. I found out later this was some politician getting time on T.V. “working” at the camp. This is happening on the local Greek news, with dignitaries, including local doctors, posing as helpers in this crisis.
The majority of refugees in the camps and on the streets are from Afghanistan and Iran, not Syria. In general, the Syrians have more money and are staying in rented apartments. Usually, those apartments are being sub-let (for a substantial profit) by other refugees. It’s a dog-eat-dog environment.
Quite a few meds. No smokable opium. No opium t all, in fact.
I saw a patient with back pain who was smoking opium for pain control. He said he didn’t want narcotics for his pain, but also said nothing else worked for him. As our clinic absolutely has no narcotics of any kind, we offered him some non-narc alternatives. He left, unhappy, then returned later, forcing his way through the scrum outside to “complain” about our “service.” Apparently narc-addiction and the behavior it engenders knows no social or ethnic boundaries.
Our clinic lead, the Persian woman who organizes these clinics (a refugee herself 15 years ago), wisely did NOT allow advertising when we started our clinic day. Just by word of mouth alone, we were nearly overwhelmed with a shouting, occasionally-pushy mass of people that formed outside our “clinic” shortly after we opened for business. HUGE credit to a great team in front of me to help control and direct the traffic outside.
The Mayor of Galatsi, and manager of the camp, is not a happy man. The Greeks dislike him because he’s helping refugees invade their country. The refugees don’t like him because he oversees a camp perpetually under-resourced. The political class over runs him, taking their own photo-ops and garnering the credit for the work being done there. When I met him in the camp, he half-shook my hand, then tersely told me to “get to work.” Can’t blame him.
I was worried to work here for a host of reasons, but I’m glad I went. I wish we could spend more time in the camps. Getting patients to our clinic at the church was a big challenge. No problem here.
I realize there is no ideal time to develop diarrhea, but surely one of the worst times is the day you also are required to learn “how” to use a Turkish toilet.





 Sometimes the greatest tragedies come quietly.
Sometimes the greatest tragedies come quietly. I think of all the people who made their living from the show too: The Almanac was written by Betsy Allister, Joy Biles, Priscilla Kinter, Heather McPherson, and Holly Vanderhaar, the program was engineered and edited by Thomas Scheuzger, Noah Smith, and Sam Hudson. Production assistance was by Kathy Roach and Katrina Cicala. I don’t know any of these people, but I presume they’re now using those fabulous writing skills on their resumes.
I think of all the people who made their living from the show too: The Almanac was written by Betsy Allister, Joy Biles, Priscilla Kinter, Heather McPherson, and Holly Vanderhaar, the program was engineered and edited by Thomas Scheuzger, Noah Smith, and Sam Hudson. Production assistance was by Kathy Roach and Katrina Cicala. I don’t know any of these people, but I presume they’re now using those fabulous writing skills on their resumes. But to my way of thinking, the greatest effect of the loss of the Almanac is to the American mind. I’ve long been suspicious of just how well the average American thinks, myself included. I’m dubious that we as a people place a high enough standard how and at what point we decide something is True. America today seems to be a land of sports spectacle and activism, neither of which lend themselves to nuanced and charitable thinking. Intellectual certainty abounds. Justice may rarely roll down like water these days, but arrogance about one’s opinions certainly does.
But to my way of thinking, the greatest effect of the loss of the Almanac is to the American mind. I’ve long been suspicious of just how well the average American thinks, myself included. I’m dubious that we as a people place a high enough standard how and at what point we decide something is True. America today seems to be a land of sports spectacle and activism, neither of which lend themselves to nuanced and charitable thinking. Intellectual certainty abounds. Justice may rarely roll down like water these days, but arrogance about one’s opinions certainly does. Realizing I wasn’t in America, where crosses are so ubiquitous they’ve become a little trite to me, I exclaimed, “You’re wearing a cross!”
Realizing I wasn’t in America, where crosses are so ubiquitous they’ve become a little trite to me, I exclaimed, “You’re wearing a cross!”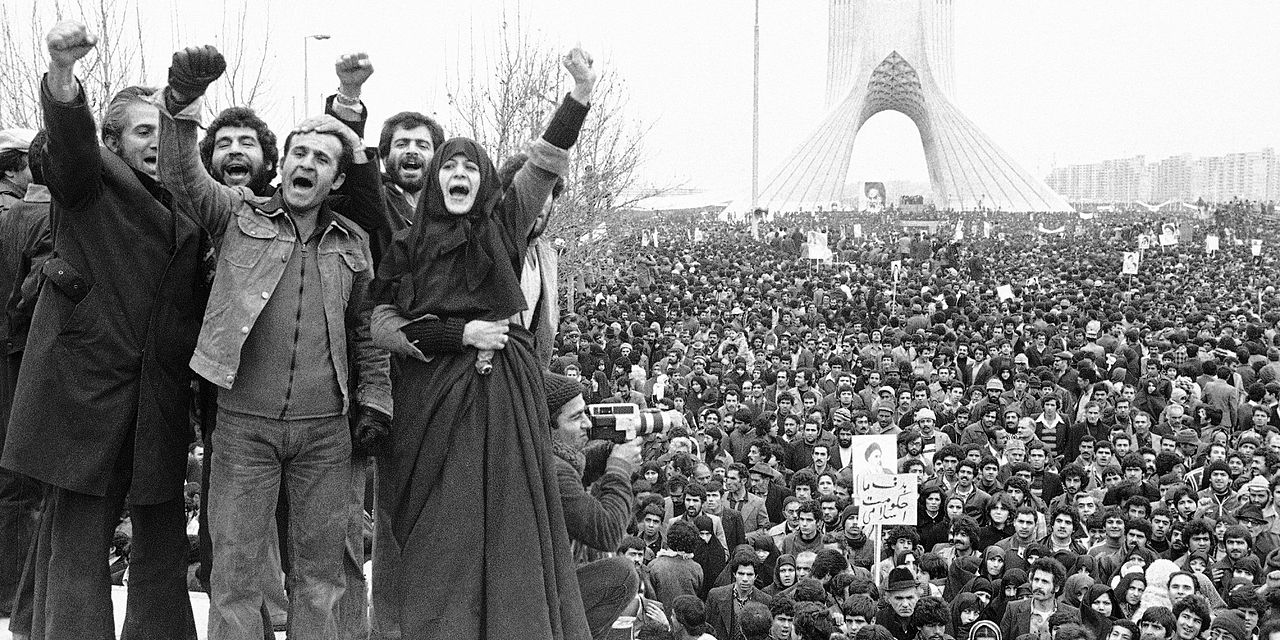

 Greek authorities soon placed this man in the Elliniko refugee camp, where he made no secret of his faith, sharing it with any around him who would listen. Not long after his arrival, a riot broke out in the camp with Muslims targeting Christians.
Greek authorities soon placed this man in the Elliniko refugee camp, where he made no secret of his faith, sharing it with any around him who would listen. Not long after his arrival, a riot broke out in the camp with Muslims targeting Christians.

 Hopefully, they can learn a bit about medical care in a refugee and/or underserved situation. As their lives are largely consumed with cheerleading, skinny jeans, teen-lit, French horn, Cello, soccer and boyfriends (ex…EX boyfriends), this might be quite an eye-opening experience for them. I hope so.
Hopefully, they can learn a bit about medical care in a refugee and/or underserved situation. As their lives are largely consumed with cheerleading, skinny jeans, teen-lit, French horn, Cello, soccer and boyfriends (ex…EX boyfriends), this might be quite an eye-opening experience for them. I hope so. It should be mentioned that most relief agencies don’t actually do any of this, even the good agencies who actually help people (lots of them are there for the photo-op and little else, it seems). I received some generous help from a professor at the London School for Hygiene and Tropical Medicine prior to my last trip, and he noted only a small number of agencies who provide care AND do good, statistical research on the populations they serve.
It should be mentioned that most relief agencies don’t actually do any of this, even the good agencies who actually help people (lots of them are there for the photo-op and little else, it seems). I received some generous help from a professor at the London School for Hygiene and Tropical Medicine prior to my last trip, and he noted only a small number of agencies who provide care AND do good, statistical research on the populations they serve.








